Vitamin K
Bronwyn Rideout - 25th May 2026
In the beginning of May, media outlets were reporting some very alarming news: more newborns were dying from bleeding, often internal. The suspected cause, however, wasn’t birth trauma, Covid, infection, or a tragic uptick in infanticide. Instead, it was due to Vitamin K Deficiency Bleeding (VKDB), formerly haemorrhagic disease of the newborn. Fortunately, it is preventable via an injection of synthetic vitamin K called Phytomenadione (or by its brand name, Konakion). The injection is given soon after birth, or the medication can be administered orally with three staggered doses over three weeks. However parental refusal has been a perennial issue with the vitamin K shot since the 1990s and, for this brief piece, I will do my best to provide an overview of the issue. Rest assured, there is no evidence of an increase in VKDB deaths in New Zealand and, in fact, there may not have been any at all. Still, parental refusal of vitamin K can contribute to declining vaccinations, a trend that was studied a decade ago and is in need of an update.
What is VKDB?
VKDB is a rare disorder that can cause brain damage and death anytime from birth up to 6 months of age. VKDB is categorised based on when it starts, and the etiology classified by whether it is idiopathic (of unknown cause) or secondary to a known cause. VKDB is described as Early if bleeding occurs in the first 24 hours. This tends to be due to maternal medications, with bleeding occurring on the scalp, skin, chest, or in the brain or abdomen. Classical VKDB occurs between day one and seven, with bleeding around the gut, umbilicus, skin, nose or at the circumcision site. Bleeding in these cases can have an unknown origin, but breastfeeding may increase vulnerability. According to the CDC, early and classical VKDB are more common, occurring between 1 in 60 and 1 in 250 newborns. Interestingly, researcher Martin Shearer wrote in 2009 that early VKDB is also rare, with the implication being that the prescribing of medications, such as anticoagulants and anticonvulsants, while not rare is still uncommon. This would have been a fair hypothesis at the time, and in a way still is today. When I started training in 2015 and became interested in maternal mental health and neurodivergence in pregnancy, advice around antidepressants and other medications in pregnancy was inconsistent, with many women today still being advised to pause such medications until after birth. Late VKDB occurs between day eight and six months, with bleeding occurring in the brain, gut, or on the skin. It is also rare, occurring in 1 in 14,000 to 1 in 25,000 infants. What makes VKDB especially scary is that there are typically no warning signs, or the symptoms may appear too late.
What is Vitamin K and why do we care?
Drawing heavily from the Wikipedia page for this whole section, Vitamin K is part of a family of vitamins that is found in food and dietary supplements. The body needs this vitamin because it modifies proteins required for blood coagulation, and also controls the chelation of calcium in bones and tissue. When vitamin K levels are deficient, uncontrolled bleeding can occur. Vitamin K is naturally present in our bodies, but for older children and adults it is also derived from dietary sources. K1 comes from plants, while K2 is derived from animal-sourced foods like chicken and eggs. Thus, a ‘normal’ diet will do the job of maintaining one’s vitamin K levels. Certain medications, and conditions that cause malabsorption of vitamin K (cystic fibrosis) or damage and disease to the liver (where vitamin K is used), can result in vitamin K deficiency.
Newborns are at an extreme disadvantage, as their clotting factors are 30-60% of adult values (~90 μg/day, 70 μg/day during pregnancy and lactation). The transfer of vitamin K from mother to newborn, in utero via the placenta or after birth via breastfeeding (which is a source of K1), is poor regardless of maternal nutrient status. However, vitamin K is also stored in the liver, and this organ is still in need of further growth and development before it can be effective at this task. Obviously, an infant cannot and should not eat leafy green salads and omelettes every day, but it is not until they commence a solid-food diet that they will begin to get adequate amounts of vitamin K and beneficial gut bacteria.

One of the arguments put forth against the universal administration of vitamin K is that the naturally low levels of the vitamin in newborns may have an as yet unknown physiological purpose. And it is true that we don’t know what this reason is. From an evolutionary standpoint, VKDB is rare enough that it doesn’t cause evolutionary pressure. This has meant that some attention has turned to modern birthing practices, especially interventions like induction of labour or caesarean sections and assisted vaginal deliveries, and has given rise to the belief that vitamin K shouldn’t be universally offered but only given to babies who had such high-intervention or traumatic births. However the research doesn’t support this stance. One study on late VKDB bleeding found no difference between mode or place of birth in rates of primary/idiopathic and secondary VKDB; the one factor all cases shared was vitamin K not being administered at birth. Another study, involving seven children, included four that were birthed in the hospital and three at home; again, all infants had not received vitamin K.
An alternative way to answer this question is to consider what happens when there is an excess of vitamin K. Well, excess vitamin K can cause anemia due to ruptured red blood cells, and can contribute to jaundice. This was true in the 1950s when vitamin K2 injections were used in 50mg doses. This older formulation is different (we now give synthetic K1) and far higher (we now give 0.5-2 mg, depending on age and route) than what we give today. According to Stanford Medicine, the current formulation can also cause elevated bilirubin levels, but only in extremely high doses (25-30mg), and impacts premature infants more than term infants; jaundice is not seen to occur due to vitamin K in newborns in standard doses. In terms of current administration practices, a midwife would have to crack open seven paediatric or three adult ampoules in order for an infant to receive 30mg at birth. Another belief about vitamin K that makes some rounds on social media is that the reason levels are naturally low is that it helps with stem cell circulation. Dr Rahi Victory, who is an Obstetrician and Gynecologist in Canada and the US, has multiple videos about vitamin K myths and explains why this particular belief does not make sense:
https://www.youtube.com/shorts/JcUQpglRCPY
Bioavailability of vitamin K from breastmilk and formula
For infants in their first year of life, the daily adequate intake of vitamin K in America is 2.0–2.5 μg/day, but there is no upper limit at this time. Breastmilk provides 0.85–9.2 μg/L, while formula is much higher at 24–175 μg/L (Formula sold in Australia by law has a minimum concentration of 30 mg/L). However, before we start throwing breastmilk out with the bathwater, if formula was guaranteed to be 100% effective in preventing VKDB, rest assured we’d be all-in as formula is simply cheaper. Over-the-counter Konakion costs approximately $12 for just five 2.0 mg/0.2 ml ampoules that each provide one dose (0.5-1.0 mg via injection, 2mg for oral) for an infant; five single-serving sachets for Aptamil Gold go for $7.19 NZD at the moment. Formula is seen to be highly protective against VKDB, but that doesn’t mean that breastfeeding is utterly ineffective. A Cochrane Study on the use of vitamin K in neonates noted that exclusively breastfed infants are also fine on 2.0 μg/day, with no evidence of VKDB. Much like the liver, however, the neonatal intestine is also functionally immature, and the mechanisms that in an adult would effectively transport and use vitamin K are reduced. Thus, the neonate’s ability to effectively utilise vitamin K from food sources is limited.
What is synthetic vitamin K?
The active ingredient in Konakion is phytomenadione, aka vitamin K1. Inactive ingredients are Glycoholic acid, sodium hydroxide, lecithin, hydrochloric acid, and water for injection. The inactive ingredients are essential for phytomenadione to be given as an injection. From Gold Coast Health:
- Glycocholic acid – Bile acid usually produced by our liver. Added to help with vitamin K absorption when given.
- Lecithin – Mixture of fats which are already found in the human body and in many foods (e.g., soybeans, egg, sunflower seeds). Added to make vitamin K dissolvable in water so it can be injected.
- Sodium hydroxide and Hydrochloric acid – Both are added in tiny amounts to ensure the injection still works after it goes through the lengthy manufacturing and supply chain process before it lands in our hospital for your baby. Also used in other medications including iron infusions.
- Water for injection – just water that is sterile (free from any bugs) that everything above is dissolved in.
The vitamin K shot is a supplement, not a vaccine. It does not trigger an immune response, or produce antibodies to prevent or combat disease. One dose of intramuscular vitamin K is effective for at least two months, while an oral dose is effective for 3-4 weeks. During this time, other forms of vitamin K are gradually accumulating in the liver and intestine. As with any treatment, supplementation, or intervention offered, there is always the possibility that the condition still occurs. When vitamin K is provided, there is still a 1 per 100,000 risk, which is far better than the 1,700 per 100,000 risk when the intervention is not provided.


How is synthetic vitamin K administered?
Administering oral synthetic vitamin K (which is the same formulation as the vit K used for injection) both overcomes the physiological limitations previously described, while also being vulnerable to them. For parents wanting a less invasive alternative, 2mg of Konakion can be administered by a midwife, nurse, or doctor orally via syringe three times over six weeks: Soon after birth, between 3-7 days postnatally, and 6 weeks after birth. While the dose of vitamin K is higher than that in breastmilk or formula, the amount is significantly smaller with the absorption happening in the mouth. It can be quite effective when given correctly, but there are risks. Spilling or vomiting soon after administration may require additional doses, as it is difficult to gauge how much was absorbed in a short period of time. Further, doses can be mistimed or missed due to parental schedules or family relocation. In some countries, the last dose may be missed if the baby is formula fed, but this is not official practice in New Zealand. Medsafe also note that there are “high risk” situations where oral vitamin K is not appropriate, including, “… maternal anticonvulsant or anticoagulant therapy (warfarin or phenindione), tuberculostatic drugs (such as rifampicin and isoniazid), prematurity, birth asphyxia or other conditions which will delay oral feeding.” Finally, neonates may simply have gastrointestinal or metabolic conditions that impede the absorption of vitamin K from the GI tract.
According to Mirone et al. (2026), these constraints may explain why intramuscular injections are seen as more effective, stating, “…administering vitamin K intramuscularly overcomes the physiological limitations of intestinal absorption, lipoprotein-mediated transport and immature hepatic uptake. This establishes a tissue reservoir that maintains sustained vitamin K availability and supports adequate γ-carboxylation of coagulation factors during the critical period of neonatal vulnerability…strategies that rely on postnatal intestinal absorption are more vulnerable in the first weeks of life”. However, Mirone et al acknowledge that such conclusions may be reflective of older studies, while newer research has found no difference between IM and oral vitamin K in preventing late VKDB, as long as everyone is compliant with the oral dosing regimen.
Parental refusal and childhood cancer
For skeptics who have been around the sun a few times, taken part in a few rodeos, and certainly weren’t born yesterday (but if you were, I hope you did get your Vitamin K jab), this is not the first time Vitamin K supplementation for newborns has been the subject of controversy. In a 1992 study by Golding et al., an association between childhood cancer and the intramuscular vitamin K injection was reported. The particular formulation Golding studied used cremophor, an emulsifier and solubiliser derived from polyethoxylated castor oil, often used for vitamins and hydrophobic drugs. While there is an increased non-significant risk of acute lymphoblastic leukaemia, subsequent studies have not confirmed this conclusion in the 30+ years since Golding’s publication. Nevertheless, this misinformation persists for vitamin K, even though the cremophor version was discontinued.
Steven Novella and Clay Jones have written/reposted some articles for Science-Based Medicine about Vitamin K refusal since 2013. In 2014, Novella described the rate of refusal as low but rising, with variations noted between hospitals and centers. Novella also noted ideology as an underlying motivator, citing the shared patterns of CAM and beliefs parents held in other aspects of their lives, such as a desire to live a natural lifestyle and refusing immunisations. A 2014 study by Gonal et al. reported that in New Zealand midwives (who were recruited from Dunedin and worked both in hospital and private practice) trailed behind other health practitioners when it came to the national vitamin K guideline, and whether all babies should receive vitamin K. Midwives, more so than doctors, would document, provide information about the injection and signs of VKDB, and educate the mother on eating a vitamin K rich diet. However, in their professional concerns midwives were less likely to think some babies were missing out on vitamin K and more likely to believe that low vitamin K levels may be a physiological process and that we are interfering with it or causing another harm.
Parents also expressed understandable anxieties around causing pain and possible allergic reactions. Indeed, haematomas and anaphylactic shock are adverse events that can occur with a vitamin K injection, but they are risks that apply to all injections. Two publications from Loyal et al in 2020 explored this phenomenon in depth. In the first article, which interviewed 17 mothers and 2 fathers, the four common themes were 1) risk to benefit ratios, especially around preservatives in the injection; 2) seeking natural approaches such as oral vitamin K or adjusting maternal intake; 3) trust and mistrust of the medical and pharmaceutical industry while turning to link minded providers, friends, and social media; 4) informed by experiences - lack of discussion around vitamin K in previous pregnancies may have motivated them to forgo this time.
In the second article, Loyal at al. reviewed several articles and found that the average refusal rate was 3.2% in hospitals, but higher in US birthing centres. Reasons for refusal identified internationally were the same as Loyal’s first article, with a noted trend that vitamin K refusal tended to occur with refusal of hepatitis B and other vaccines.
The ProPublica article that appears to have sounded the first klaxon about this trend wasn’t just sharing anecdotes; it was backed by evidence. An analysis of 5 million births in the United States between 2017 and 2024 found that nearly 200,000 (3.92%) did not receive the vitamin K injection. On a by year basis, injection refusals increased from 2.92% in 2017 to 5.18% in 2024. Highest rates occurred with vaginal births, as well as in non-Hispanic white populations and groups where race/ethnicity was unreported or reported as “other”.
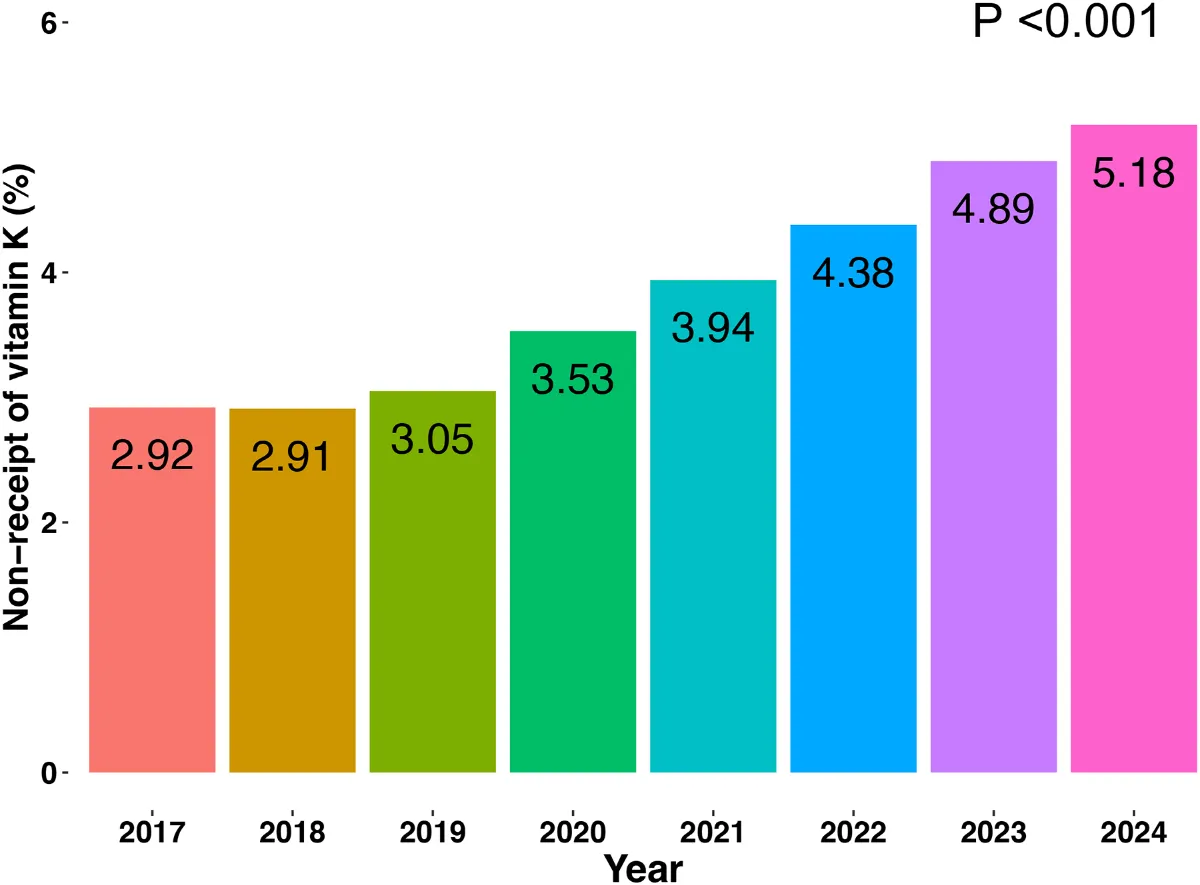
Source: Percentage of newborns not receiving prophylactic intramuscular vitamin K administration after birth in Scott et al. (2025).
Duaa Eldeib, writing for Propublica, reported that following the first rumblings of parental refusal in 2013/2014 there were multiple efforts across the US to counter misinformation and address parental concerns. As one interviewee put it, the success of those efforts and the subsequent wind-down may have contributed to the increase in refusals, as the public underestimated the severity of the disease. Health literacy around vitamin K remains a major obstacle, as demonstrated by one grieving father:
A third family, who made their decision after reading about vitamin K on social media and talking with their midwife, dismissed the vitamin K shot altogether. Instead, the father expressed outrage at the hospital for not delaying the clamping of the umbilical cord. He said he believed doing so would have allowed his son to be infused with vitamin K from the cord blood, a popular theory on social media. Research, however, shows that while delayed cord clamping can raise the baby’s hemoglobin levels, it does not have the same effect on vitamin K.
“I figured the hospital was already pissy with me because we didn’t vaccinate at all,” he told ProPublica. “They lost out on all the money from that.”
The family’s anger has subsided some since the baby’s death, in part because of their trust in God’s plan.
“I can sit here and be upset and sad, but this brought me closer to God,” the father said. “I just can’t wait to be with him.”
But Eldeib also suggested that US doctors and hospitals may also be in the dark. In hindsight, failing to start tracking vitamin K refusal in 2013 may have been a missed opportunity. It is doubtful that the American government, which most likely has the resources to commence such research, will start tracking under the current administration. Further, addressing this issue post-Covid, while still necessary, is akin to being the ambulance at the bottom of the hill.
Final thoughts
There is no evidence or chatter in New Zealand media as to whether this is an issue that we should be aware of over here. At present, there is no current data on vitamin K uptake and possible connections to subsequent vaccine refusal in Aotearoa. While administration of vitamin K is data that is captured in all birthing units, as well as by midwives in New Zealand, there hasn’t been an update that consolidates DHB level data with stats from homebirth midwives and broader vaccination trends from 0 to 12 years old. The Perinatal and Maternal Mortality Review Committee (PMMRC) would be the best chance to track any deaths or impairments due to VKDB, although the reviews are often a couple of years out of sync when published. In the 2024 report, which covered 2021 data, there were 191 neonatal deaths among 58,659 live births. VKDB is not explicitly mentioned in the perinatal death classification they provide but, as of 2021, New Zealand is at least not seeing the morbidity trends that are the subject of concern in the US.
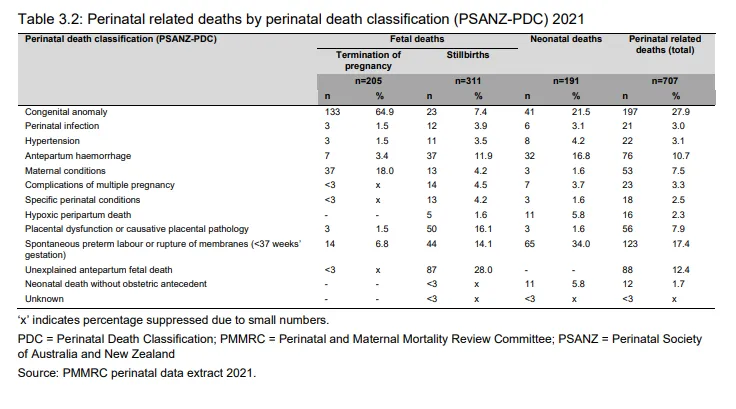
Source: Sixteenth Annual Report of the Perinatal and Maternal Mortality Review Committee
Two studies were published in 2015 that focused on issues around vitamin K in Dunedin. One by Burke et al reviewed birth records from a single tertiary birthing unit in Dunedin.
(For international readers, the term birthing unit is not inherently synonymous with birthing centre. As per the New Zealand College of Midwives, tertiary and secondary facilities, “… provide care for women who may have complex medical or pregnancy complications, and who may require specialist care alongside their midwifery care. These facilities have caesarean section capabilities. There are obstetric, anaesthetic, paediatric, midwifery and nursing services available in tertiary facilities”.)
Anyways, in Burke et al. the records of almost 7,100 mothers and babies from 2009 to 2012 were reviewed. Approximately 93% received the intramuscular injection, and 5.4% received oral. Refusal was associated with Asian/Indian ethnicity, vaginal birth, and gestational age, while uptake of oral vitamin K was similarly associated with those factors, along with obstetric nurse as the lead maternity carer (LMC), and LMC experience per decade. However, even in 2015, there was a noted drop in injection uptake, from 96% in 1998-2008. Bernhardt et al., which looked at records for babies born at a tertiary unit in Dunedin from 2010-2011, found that 92% of 3,575 babies received the injection, and 5% received it orally. Both the choice of orally administered vitamin K, and a declining rate of allowing vitamin K to be administered, were associated with declining some or all immunisations. 17% of parents who declined vitamin K also declined all other immunisations, compared to 1.2% who consented to vitamin K and later declined some vaccinations. Of those that received oral vitamin K, 5% did not immunise, compared to the 1.2% of families that consented to the injection and later declined immunisation.
Thus, things are looking incredibly favourable for New Zealand babies, but the research is in dire need of an update, especially in light of the Government’s Covid-19 response. Decision-making around vitamin K is a component of perinatal and midwifery care in New Zealand, but health care practitioners are not the only ones who can influence parents’ decisions. Friends, family, and media all play a role, and skeptics with loved ones who are pregnant shouldn’t underestimate the power of listening and information sharing. If there is a baby in your family or social circle that hasn’t received vitamin K, keep these symptoms in mind as they require urgent referral to their health care provider. From Kids Health:
- easy bruising
- increasing bruising around their head and face
- bleeding from the nose, gut or umbilical cord (bleeding and bruising are not normal in the first months of life)
- being irritable, vomiting, having paler than usual skin or (for dark-skinned babies) pale appearing gums - these might be due to internal bleeding
- any signs of worsening jaundice in pēpi over 3 weeks old